
















Ministry of Health CS Aden Duale appeared before Parliament on Wednesday to account for the country’s Ebola preparedness, reassuring Kenyans that 22 suspected alerts were investigated across 9 counties, every single one testing negative.
The counties flagged included Nairobi, Kiambu, Uasin Gishu, Nyeri, Nakuru, Nyamira, West Pokot, Kisumu, and Bungoma. The results are the product of a surveillance architecture that Kenya has spent years building and which is now being stress-tested in real time.
At the time of reporting, the Bundibugyo strain of Ebola has torn through DRC’s Ituri Province and crossed into Uganda, prompting the WHO to declare it a Public Health Emergency of International Concern on May 16.
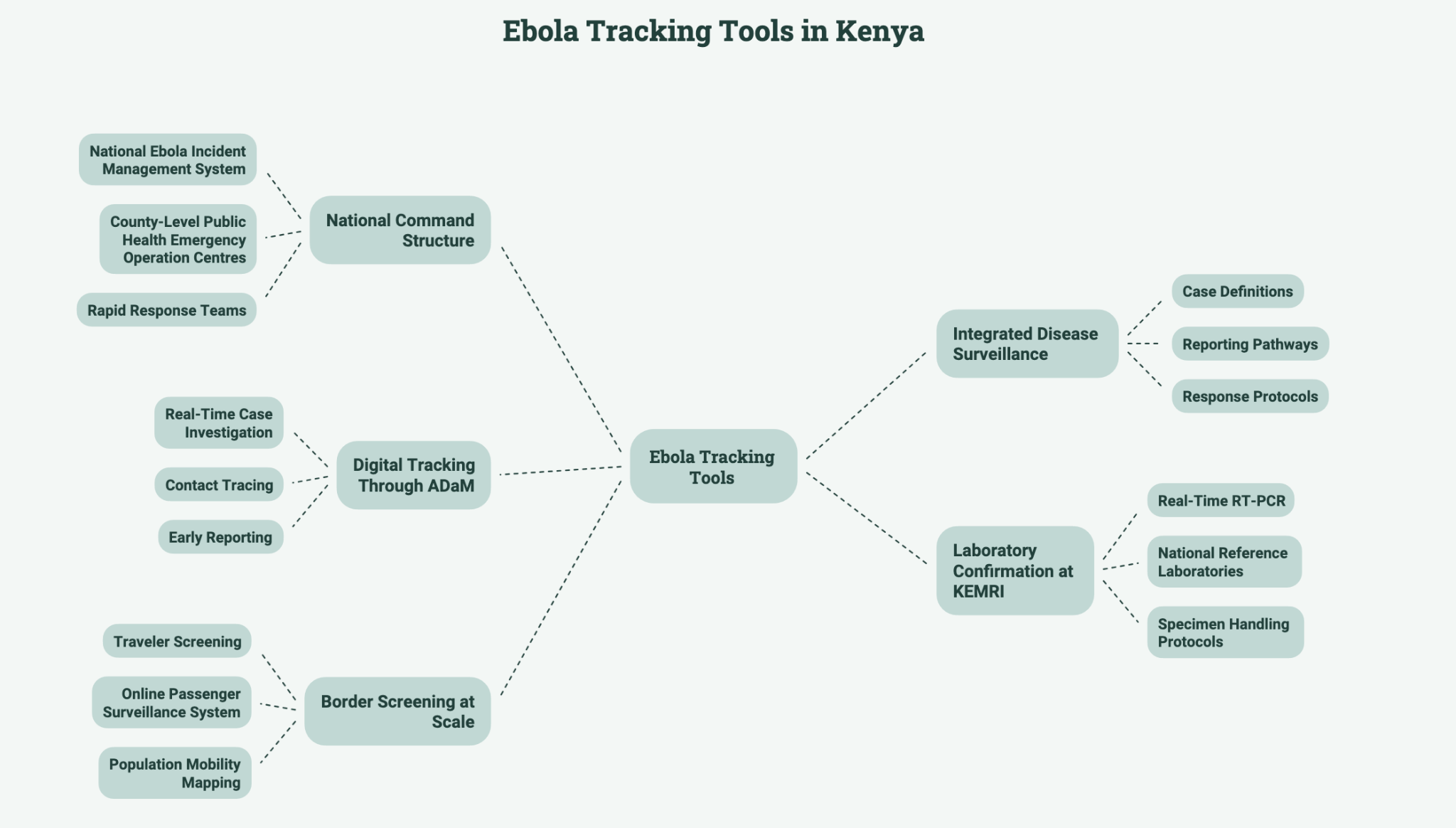
A National Command Structure
The starting point is the National Ebola Incident Management System, activated on May 20 to provide a unified central command and coordination framework.
It sits above county-level public health emergency operation centers, all kept on high alert, creating a clear chain from a rural health worker flagging a suspected case all the way to national decision-makers.
When an alert is raised, rapid response teams are placed on standby for immediate deployment. These are multidisciplinary units combining epidemiologists, clinicians, and laboratory personnel, trained specifically for outbreak conditions.
Integrated Disease Surveillance
The broader scaffolding is Kenya’s Integrated Disease Surveillance and Response framework, the national adaptation of a WHO regional strategy that runs surveillance across every tier of the health system, from rural dispensaries to national referral hospitals.
It defines the case definitions health workers use to identify a suspected Ebola patient, the reporting pathways that carry that alert upward, and the response protocols that follow. Advisories have been issued to all 47 counties to ensure uniform vigilance regardless of proximity to the border.

Digital Tracking Through ADaM
The digital layer is less visible but crtical. Kenya, in collaboration with ICAP at Columbia University, developed the All-Disease Outbreak Module (ADaM), an electronic platform built for real-time case investigation, contact tracing, and early reporting.
ADaM gives frontline health workers a structured tool for logging and escalating alerts rather than relying on phone calls and paper records. The speed this enables matters considerably with a hemorrhagic fever, where the window between exposure and rapid deterioration is narrow.
Laboratory Confirmation at KEMRI
Surveillance is only as good as what happens after the alert. The Kenya Medical Research Institute (KEMRI) has confirmed it has the capacity, infrastructure, and trained personnel to diagnose Ebola and is recognized by WHO as a sub-regional reference laboratory.
Samples are processed using real-time RT-PCR, the molecular gold standard for detecting Ebola RNA in clinical specimens. Kenya’s national reference laboratories operate around the clock to support this, having strict specimen handling protocols so as to govern their safe movement from the point of collection.
Border Screening at Scale
At the points of entry, more than 34,500 travelers have been screened, including over 18,000 international passengers, truck drivers, and conveyances.
An online passenger surveillance system has been deployed, and population mobility mapping is underway in high-risk border areas.
A risk point to note is that DRC and Uganda share long and porous borders with East Africa’s road freight network, and Kenya is the region’s primary commercial transit hub.
The Laikipia Question
All of this sits against a politically charged backdrop. The proposed US quarantine facility at Laikipia Air Base has drawn sharp opposition from Kenyan doctors and civil society, with the High Court temporarily halting the arrangement.
The facility is intended to treat Americans exposed to Ebola in DRC, with the US deploying physicians, nurses, laboratory technologists, and mental health professionals with prior Ebola response experience.
Duale’s defense before Parliament was blunt, stating that the thousands of Kenyan truck drivers and cross-border traders moving through the region every day represent just as real a risk as the Americans the facility would formally serve.
Wednesday’s briefing ultimately demonstrated that Kenya’s surveillance system is not merely reactive. It is generating alerts, investigating them rapidly, confirming negatives, and feeding results back into a central command structure, all without a single confirmed case.
That is the system working as designed. The test, should a positive ever come back, will be considerably steeper.













{kind=link}